Detecting oral cancer - the exam review
Detecting Oral Cancer: A Guide for Health Care Professionals
A thorough head and neck examination should be a routine part of each patient dental visit and general medical examination. Clinicians should be particularly vigilant in checking those who use tobacco or excessive amounts of alcohol.

II. Perioral and Intraoral Soft Tissue Examination



BUCCAL MUCOSA: (Figures 5 and 6) Retract the buccal mucosa. Examine first the right then the left buccal mucosa extending from the labial commissure and back to the anterior tonsillar pillar. Note any change in pigmentation, color, texture, mobility, and other abnormalities of the mucosa, making sure that the commissures are examined carefully and are not covered by the retractors during the retraction of the cheek.


TONGUE: (Figure 8) With the patients tongue at rest, and mouth partially open, inspect the dorsum of the tongue for any swelling, ulceration, coating, or variation in size, color, or texture. Also note any change in the pattern of the papillae covering the surface of the tongue and examine the tip of the tongue. The patient should then protrude the tongue, and the examiner should note any abnormality of mobility or positioning.

(Figure 9) With the aid of mouth mirrors, inspect the right and left lateral margins of the tongue

(Figure 10) Grasping the tip of the tongue with a piece of gauze will assist full protrusion and will aid examination of the more posterior aspects of the tongue lateral borders

(Figure 11) Then examine the ventral surface. Palpate the tongue to detect growths

FLOOR: (Figure 12) With the tongue still elevated, inspect the floor of the mouth for changes in color, texture, swellings, or other surface abnormalities.

PALATE: (Figures 13 and 14) With the mouth wide open and the patients head tilted back, gently depress the base of the tongue with a mouth mirror. First inspect the hard and then the soft palate.

(Figure 14) Examine all soft palate and oropharyngeal tissues

(Figure 15) Bimanually palpate the floor of the mouth for any abnormalities. All mucosal or facial tissues that seem to be abnormal should be palpated

Oral Lesions Suspicious for Oral Cancer
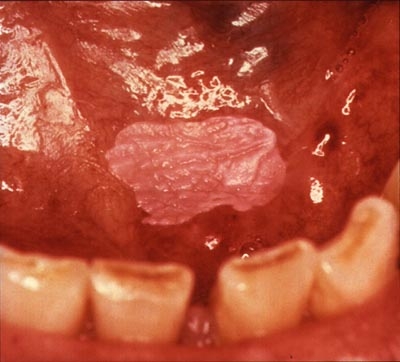
Homogenous leukoplakia in the floor of the mouth in a smoker. Biopsy showed hyperkeratosis

Clinically, a leukoplakia on left buccal mucosa. However, the biopsy showed early squamous cell carcinoma. The lesion is suspicious because of the presence of nodules

Nodular leukoplakia in right commissure. Biopsy showed severe epithelial dysplasia

Erythroleukoplakia in left commissure and buccal mucosa. Biopsy showed mild epithelial dysplasia and presence of candida infection. A 2-3 week course of anti-fungal treatment may turn this type of lesion into a homogenous leukoplakia.
Revised March 2011